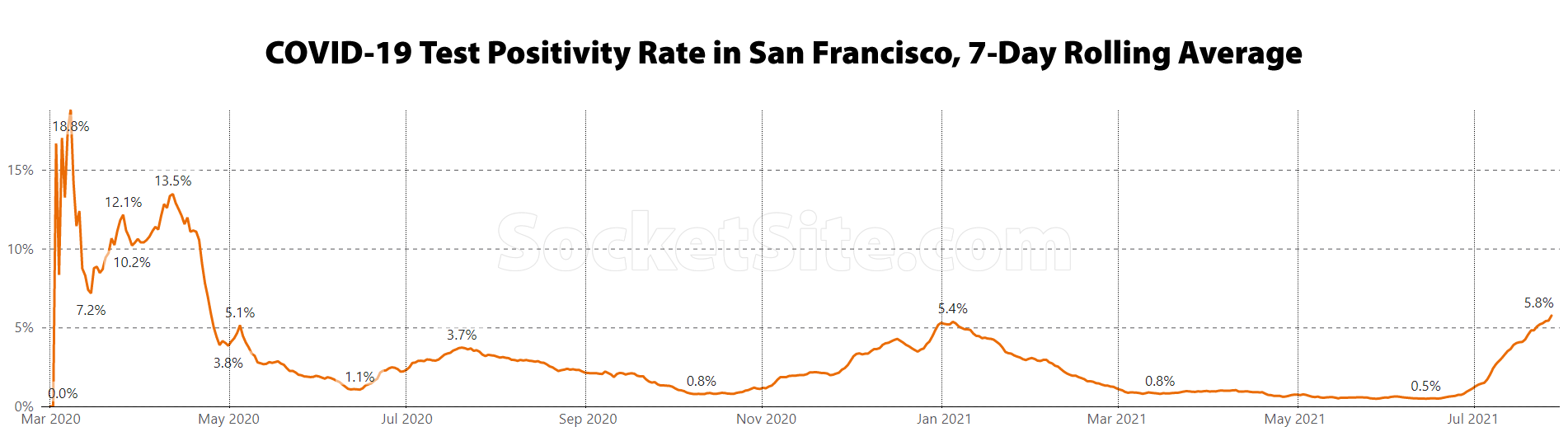
The COVID-19 test positivity rate in San Francisco just hit 5.8 percent, which is significantly higher than the 3.7 percent positive rate at the peak of the first wave, in July of 2020, higher than the 5.4 percent positive rate at the peak of the second wave in January of this year and the highest average positivity rate since April of 2020.
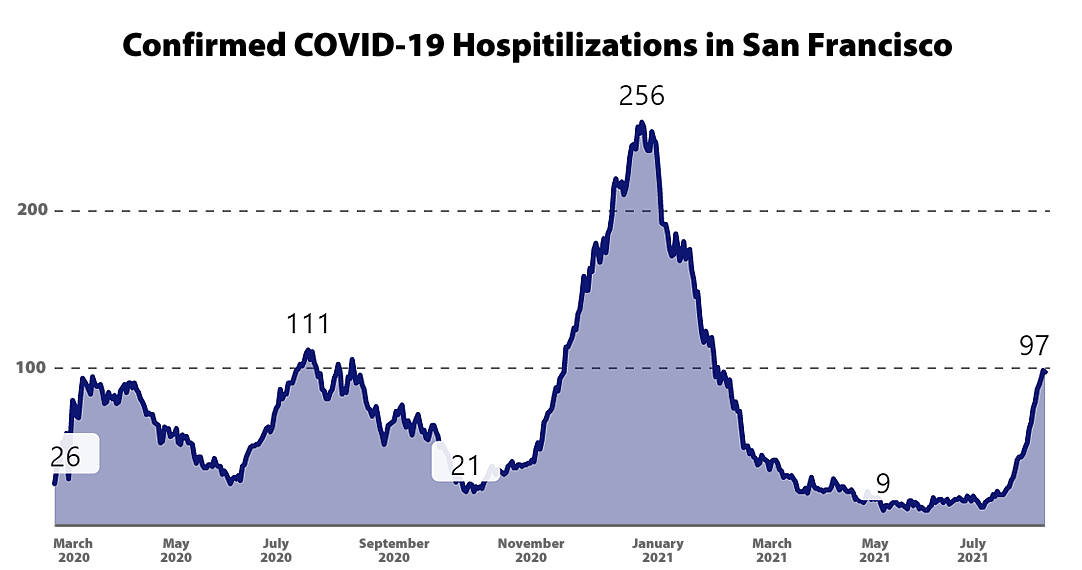
With the ramp in spread, primarily amongst the unvaccinated, the average number of daily new COVID-19 cases in San Francisco has spiked to 235, which is over 80 percent higher than at the peak of the first wave and versus an average of less than 15 new cases per day this past June. And while hospitalizations lag case rates, there are now 97 hospital beds occupied by Covid-19 patients in San Francisco, including 28 people in an ICU. There were 111 hospitalizations at the peak of the first wave in 2020.
UPDATE (8/6): The COVID-19 test positivity rate in San Francisco is up to 6.2 percent, the average number of daily new COVID-19 cases in San Francisco has jumped to 265 and there are now 100 hospital beds occupied by Covid-19 patients in San Francisco, including 33 people in an ICU, which is the most in five months.
UPDATE (8/13): COVID-19 Hospitalizations Hit First Wave High in San Francisco
While the positivity rate could potentially be a great leading indicator, it is tainted by human behavior, making it not a true random sample. Since samples are overwhelming from voluntary tests, the mood of the public can affect results. When there is high anxiety over covid, more people with borderline symptoms will take the test, lowering the positivity rate due to a higher number of non-infected people being tested. When there is less anxiety, the proportion of people tested shifts more towards those with severe symptoms, increasing positivity.
A more accurate measurement would benefit from a true random sample of the population that factors out human behavior.
But once again, “the average number of daily new COVID-19 cases in San Francisco has spiked to 235, which is over 80 percent higher than at the peak of the first wave and versus an average of less than 15 new cases per day this past June” and with 97 hospital beds now occupied by Covid-19 patients in San Francisco, including 28 people in an ICU. There were a total of 9 hospitalized COVID-19 patients in San Francisco in mid-May.
I’m not denying a resurgence of cases, just pointing out that test positivity rate has a flaw and could be improved.
It may be misunderstood by a certain number of people, but I’ve always understood it represents the percent of positive tests among those who are tested, as opposed to the general population. Perhaps public health officials should talk about that more, but clearly, a rising positivity rate isn’t good news.
UCSF conducts tests on all patients coming in for any elective surgery, not simply for covid testing, and tracks this. that positive % number has also gone up > 5x. it’s rampant
Thanks Jimbo. The elective surgery group is much closer to a random sample.
UCSF isn’t just testing people coming in for elective surgery, though. I had an elective procedure at UCSF and got my test for that. Then 2 days after the procedure, I was notified by UCSF that, while there, I had been exposed to covid and I requested and got another test a week later (which was negative). Shortly after, there were news articles about staff at both UCSF and SF General being positive and exposing staff and patients. So to a certain extent UC is also testing, at the same site, people who have reason to think they are positive because of known exposure.
Incidentally, I explored other ways to get tested and found them few and difficult. Things have changed since last winter. Now in San Francisco you have to go pretty far out of your way to get a test which means only people worried they have covid or who think they were exposed are probably getting tested. This also has an impact on sampling.
There are no random samples in clinical research. All who are tested have reason to suspect or worry that they may be infected, thus making them distinct from those without such motivation. I don’t know how one would “improve” a statistic based on a clinical sample. This is research 101.
The metric should be deaths, now that vaccines are available, me thinks. We are going to have to get used to living with Covid.
Deaths typically lag hospitalizations by a month or two. And having dropped to a total of 5 in June, there were 7 COVID-19 deaths in July for a cumulative total of 565 confirmed COVID-19 deaths in San Francisco since the start of the pandemic.
mutliple metrics: cases, case positivity, long covid, hospitalization, ICU and deaths. all are very important to measure the impact of the virus. the only outcome is not death or no death
Not counting deaths anymore as they have declined greatly thanks to the vaccine. So they have to switch the metric up so we can continue to live in fear.
How many deaths in SF related to homicide? Drug overdose? Preventable disease?
While deaths, which are projected to climb in the upcoming weeks, are certainly one important metric to track, hospitalizations, which represent intensive uses of scarce resources, are another.
In addition, a rise in the spread increases the likelihood of further, more deadly, mutations.
And unlike COVID, crime, drug use, heart disease and cancer aren’t communicable diseases against which one can be vaccinated or help prevent being spread and/or contracted by simply wearing a mask as prescribed.
How about student population of SFUSD * normal hours of instruction per day * scheduled days of instruction lost since March 2020.
That’s data we should be tracking.
Times the hours wasted on school renaming by the Ess Eff Board of Education
“Not counting deaths anymore as they have declined greatly thanks to the vaccine.”
The thing is that the vaccine only helps those who take it. And since breakthrough cases are rare, I assume that most cases are among the unvaccinated. So I think that the issue is that among the unvaccinated cases, hospitalizations and deaths will most likely follow the pattern, with the lag that the editor indicated, that we’ve seen before.
There has been some conflicting reports, but the CDC report that just leaked indicated a worse prognosis for Delta vs the ancestral strain (though we might be better at treatment now). I think this is something to be taken seriously.
Breakthrough cases are not that rare. It’s hospitalized breakthrough cases that are rare.
Israel now says the Pfizer vaccine is only 39% effective (name link) and I’ve seen reports that the majority of positive cases in Israel are breakthrough cases.
The reason we are not living in fear in SF is because SF has taken strong anti Covid measures.
In the last 16 months, at least 600,000 Americans have died of Covid. In that same time frame, about 120,000 Americans have died of drug overdoses. Both are tragedies, but Covid is clearly killing more people.
SF (and the Bay Area) jumped on this fast. But the culture of under reporting covid cases and deaths advanced by many conservative governors (and even some countries like Brazil and India) suggests that 600K+ US figure may be quite low.
Do you lock the front door of your house? Is that living in fear, or taking prudent precautions?
Yes I lock my front door. But I don’t spend every waking moment worrying that someone may break in or steal property (both of which are far more likely than dying from COVID as a fully vaccinated individual).
So it’s a prudent precaution, good. No one mentioned fear excerpt for you, apparently exponential curves are not calming. But you are probably referring to the media circus which is really just click driven advertising, that important issue you should take up on another forum as it touches (hurts?) many more aspects of our lives.
COVID is never going away.
Everyone is either catching the virus, getting vaccinated or both.
COVID is a tiny problem for the vaccinated.
San Francisco has vaccinated effectively all the 12+ that want it.
Now, the virus is working its way through the rest.
Here, here!
The rest includes kids under 12. That is the problem and why everyone should still be doing there part to combat the spread.
Who said anything about not doing their part?
While I do hope vaccines are approved for under 12s soon, if you look at the numbers, the risk of COVID for under 12s is WAY down the list of other potential dangers they face.
According to the CA COVID information site, the total CA COVID deaths for the 0-17 age group rounds to 0%.
Let’s see, so you as an armchair epidemiologist are saying:
– if something is down on a list it doesn’t matter
– vaccines are perfect forever
– risk of a still novel virus and novel strain round to 0%
– the virus is a static object that you can control
– kids can be infected and infect others included in vaccinated, new strains be damned
– kids can be in ICU and have long term effects as long as they don’t die
– same for anyone infected via infected kids
– we are 100% accurate in attributing and accounting for COVID outcomes
Also all causes of death for under 17 round to 0, not a useful comparison.
protecting kids should be of utmost importance, and hospitalizations (leading indicator) for kids is going way up in the areas in the southeast where cases are rampant. delta seems to be worse for all, including kids
Protecting all kids from a failing educational excuse system is much more important than saving one asthmatic kid out of a million. America is becoming more stupid with each classroom day lost.
^ Just so everyone is clear here, you are actively in favor of getting kids with pre-existing conditions killed or burdened with long term effects because you think classrooms should operate in a totally unmodified pre-pandemic fashion.
wow soccermom. i’m all for kids being in school and support requiring all school staff to be vaccinated. but protecting kids from long covid, hospitalization and death is of utmost importance. those don’t have to run counter to each other. mandating vaccines for all will take care of both problems
The news about Delta has made the school district’s excess of caution look a lot smarter than it did a month ago.
Hey Never in Doubt,
As a medical expert, what are the long term consequences of Covid in children?
My bad!
Shouldn’t have mentioned kids!
Let’s recap.
COVID is *never* going away. There is no finish line.
Once all age groups can be vaccinated, the constituency for continuing mandates of any kind will be irrelevantly tiny.
No argument that once everyone, including 0-12 kids, is vaccinated, our response to Covid will look different. Of course, once we’re all vaccinated, Covid will also look very different. Until then, we all still have to act together to fight it.
Hospitalization data is useless unless your know percentage with preexisting conditions (or unvaxxed). We are back to fear mongering with incomplete data.
This may evolve to a never ending pandemic. I’ve stated (on this forum) before the vaccines became publicly available and I’ll state it again. The virus will mutate (it already has several times) either on its own or by way of human intervention. Unless vaccines which grant sterilizing immunity are developed, this virus will continue to evade any and all vaccination regimes. None of the vaccines today grant sterilizing immunity. Also none of the vaccines today protect against upper respiratory infection — the trouble starts when it propagates into lower respiratory system and immunity is not strong enough.
As long as the virus can infect upper respiratory system (which it can – almost everyone), it will keep mutating. Frankly, leaky vaccination in the face of a pandemic is a recipe for disaster since it forces the virus to selectively evolve to escape vaccine and become deadlier — which it appears is already happening.
The hope is that (in general) as viruses turn more virulent they tend to get less deadly. Lets hope that is the case with this one too.
“selectively evolve” No. It doesn’t have a conscience. It’s just a random virus, that given the chance will evolve. It might devolve into something less contagious or almost harmless, or it might become more harmful.
Any virus that has enough hosts will continue to change, not intentionally, but by accident. If enough people get inoculated, it will have no where else to continue to change.
I haven’t heard a single person ever say that if everyone in SF gets vaccinated the disease will go away.
I hope you are not being blunt on purpose. Evolution is a process that ‘selects’ towards fitness and survival.
For a virus, fitness is its ability to propagate within a host and survival is its ability to transmit to as many hosts as it can.
Lethality is incidental. It is not necessary that lethality is down or up regulated by selective pressure. It can be one or other or both. This much is already evident in various Covid strains.
You are incorrect. Evolution doesn’t have a conscience. Evolution is a process of genetic mistakes. An evolutionary mistake that adds an advantage may be passed down to following generations, giving that lineage an evolutionary advantage.
Covid-19 is not strategizing, it isn’t selecting anything. It’s just randomly jumping from host to host, making genetic mistakes along the way. Evolving negatively or positively or in ways that will make no noticeable difference. Given enough hosts and time, eventually one of these genetic mutations will cause great damage to humans. If it has nowhere to evolve it will end.
@Bluntcard – the process of accumulating a relative and specific genetic advantage by random mutation and passing it on to next generation is called “selectivity”. Conditions (environmental or other) that coax outcomes is called “selective pressure”.
If you happen to be infected with Covid, among the numerous mutation that may arise, the most advantageous mutant in terms of fitness and survival is ‘selected’ to dominate the other mutants.
This selection happens not because the virus has a “conscience” (as you seem to hinge on) but rather it is the most advantageous next evolutionary step for the virus.
This selection happens in every species. Though in virus, the rate of mutation/selection can be very high given a large replication/mutation surface such as a global population.
You can read a little bit about it here: The role of selectivity of the SARS-CoV-2 virus for human genetic profiles in susceptibility and resistance to COVID-19.
Lotta people out here eager to trot out “fearmongering” and reasons why a big spike in cases shouldn’t be mentioned, much less acted upon in any way. That’s what my COVID-denying, anti-vax relatives say too. Look, don’t be extreme, but maybe don’t scoff at data just because it implies bad news.
Will this resurgence lead to even more office vacancies? Lower apartment rents? Even more Lumina unit price cut carnage?
I think the return to work and cities is postponed a little longer. Be safe socketeers!
UPDATE: The COVID-19 test positivity rate in San Francisco is now up to 6.2 percent, the average number of daily new COVID-19 cases in San Francisco has jumped to 265 and there are now 100 hospital beds occupied by Covid-19 patients in San Francisco with 33 people in an ICU. Once again, there were 111 hospitalizations at the peak of the first wave in July of 2020 in San Francisco, a number which should soon be surpassed.
Per the CDC today “Weekly Updates by Select Demographic and Geographic Characteristics”), total cumulative COVID deaths in California for ages 0-17 is 37. Compare that to 4,744 deaths from all other causes since the beginning of the pandemic. In other words, a person aged 0-17 is 128 times more likely to die from anything other than COVID. Driving in a car is far more dangerous to that cohort than the virus.
Very sad how easily people can be manipulated by fear.
Dear Dr. Another anon,
What are the long term effects of Covid in children?
While the odds of a youth dying from the current variants of COVID-19 are extremely low, which is neither new nor contradictory information, unfortunately that doesn’t translate into a reduced risk of a youth spreading the virus, both within and beyond the youth cohort.
In addition, allowing the virus to spread unchecked amongst healthy youths is likely to exacerbate the adaptation, evolution and further strengthening of the virus beyond the virulence of the delta variant.
So strange that the opinions here seem to represent the extremes – “it’s all overblown, kids will be fine, not a problem” vs. “kids will die, long covid, eternal illness” – when the reality (as always) is somewhere in the middle. Vaccines work, but not perfectly, so let’s get as many people vaccinated (though workplace mandates, other incentives), and then take moderate measures (e.g. indoor masking, masking in schools) to protect the vulnerable and mitigate runaway infections in the general population.
I am constantly amazed at our abilty to make this far more complicated than it really needs to be. Somehow reasonable measures we take for granted in other parts of our lives (e.g. mandatory vaccination for measles in schools, seatbelt/helmet laws) seem to engender a “sky is falling” attitude around this disease.
But isn’t a worldwide epidemic now approaching 2 years with no end in sight rather extreme?
unfortunately the irrational exuberance illlogic has to be countered with reality and expectations going forward …
Also what does it mean that ‘vaccines work but not perfectly’ — all that really means is that they are not good enough to prevent infection and hence still ample ground for virus to infect and hence mutate. That was one of the many poor messagings we got from the government which effectively said vaccines are perfect and if you vax this is over. Increasingly that looks untrue …
I guess people were also tired of hearing about WWII, at least in the US? But it didn’t make it go away until things went nuclear …
the government saying the vaccines work perfectly is as true as needing to bomb Japan to end the war. I guess you got that part right. “countered with reality” indeed
I never heard from any government source that the vaccines worked perfectly. That is serious misunderstanding…for partisan or anti vaxxer nonsense reasons
what does this have to do with real estate?
As long as the resurgence doesn’t have any impact on return to office plans, eviction moratoriums that are slated to expire, a potential rollback of San Francisco’s reopening and local employment, all of which impact the demand for housing, office and retail space, along with the collection of rents, not much.
Yeah, I mean what’s the chance THAT could happen?
Speaking of which: Delta Variant Stalls the Economic Recovery in San Francisco
I can’t quite parse you there … I’m sure that nuclear bomb was not a light decision but did involve years of planning and concerted effort to prevent considerable greater tragedy (with millions dead already). Feel free to develop that analogy deeper … pandemic is war, not a time for everyone to push to ease/cancel/shame/ridicule restrictions to get on with their frivolous life.
How about this, how many people in Bay Area know they are in an ‘area of substantial or high transmission’? Which requires many specific behaviors for vaccinated now (as opposed to a month ago).
Nuanced and evolving guidelines are not falling on fertile ground.
I wonder how many people getting tested these days and showing positives are vaccinated. Because last year nobody getting tested was vaccinated. So then other questions come into play, such as the number of asymptomatic positives, positives showing mild symptoms, or positives with covid symptoms that don’t require hospitalization. Also what percentage of those hospitalized are infected with the delta variant and are not vaccinated, etc.
Remember when Covid first broke out? Everyone smart was saying vaccines are years away, if ever? The idea way back then was to slow down the spread so as not to overwhelm the hospitals on the way to herd immunity. Science tell us everyone who is infected and recovers will have a durable immunity. So between the vaccinated and recovered the Delta variant will burn out in two to three months. See India where in three months we saw a 10x decline also see UK
“Science tell us everyone who is infected and recovers will have a durable immunity.”
Unfortunately, that is not what science tells us. What science actually tells us is that most people who were infected have partial immunity.
It is true that is what they said early on while adding we don’t know how long natural immunity will last. Well we now know it is quite durable. Perhaps more durable than the vaccine. Israel one of the first and most successful countries to get “fully” vaccinated are discovering that its effectiveness of the vaccine is waning. Up to 85% of hospitalizations for Covid are patients that are fully vaccinated according to Dr. Kobi Haviv—Director of the Herzog Hospital in Jerusalem, Israel so yes compared to vaccinations natural immunity is durable.
You said that “everyone who is infected and recovers will have a durable immunity”. That is what I am pointing to, and that is not true, unfortunately. Previous infection confers some immunity to most people, but it does not confer durable immunity for everyone.
But if you want, feel free to argue about the meaning of “durable”.
Vaccine or not – ultimately the quality and quantity of anti-body response depends on the robustness of the individuals immune system and inflammatory response.
Just because someone got a vaccine (or recovered from an infection) doesn’t guarantee robust immune response – the individual must do their part in keeping their immune system in tip-top shape.
The most important factor in fighting Covid is NOT the robustness of the person. It is whether the person has been vaccinated.
From a summary of the actual Israeli study on the durability of the Pfizer-BioNTech BNT162b2 vaccine:
“Using 146 days [after being fully vaccinated] as their cut-off, the researchers found that within the 60 and over age group, 2.19% of vaccinated individuals tested positive for SARS-CoV-2. Comparably, the positivity rate in the 40-59 and 18-39 age groups was 1.93% and 1.39%, respectively.”
The vaccines work and are durable.
Indeed, not ignoring the 1/500 chance of not recovering, one could also endure lasting and debilitating symptoms and if oxygen deprivation was involved even an IQ drop …
Unfortunately it is not ‘the flu’ and we still have lots to learn. We should also not ignore the fact that all our best data comes from unified health systems like Israel and UK…
Update on durability of the vaccine:
As you may recall, last month Jerusalem Post reported that of the 143 covid patients admitted to the hospital, there were more fully vaccinated patients than the unvaccinated. Of this figure, 58% were fully vaccinated while 39% were unvaccinated.
Now, the situation in Israel is getting worse for fully vaccinated people. In an interview with Israel Channel 13, Israel top health official Dr. Kobi Haviv, who is also the Director of the Herzog Hospital in Jerusalem, says:
“95% of the severe patients are vaccinated. 85-90% of the hospitalizations are in Fully vaccinated people. We are opening more and more COVID wards. The effectiveness of the vaccine is waning/fading out,” Dr. Haviv said.
He went on to say that, “90% of severe covid hospitalizations are fully vaccinated,” he noted. Unfortunately,’ explains the Director, the effectiveness of the vaccine is ‘fading,’ “outbreaks in hospitals, one patient infects a large number of people, it is no just here and there,” he added.
From a summary of the actual Israeli study on the durability of the Pfizer-BioNTech BNT162b2 vaccine:
“Using 146 days [after being fully vaccinated] as their cut-off, the researchers found that within the 60 and over age group, 2.19% of vaccinated individuals tested positive for SARS-CoV-2. Comparably, the positivity rate in the 40-59 and 18-39 age groups was 1.93% and 1.39%, respectively.”
The vaccines work and are durable.
I couldn’t find a single reputable news organization that reports JtK’s article, but on the other hand it appears that the effectiveness of the vaccine may be waning: probably from a new slightly varied strain. A hospital in Colorado is now noting that the vaccine has only prevented 79% of hospitalized cases, which is down from the 95% that was originally reported and appears to be 89% for other counties. They note that the county’s vaccination rate is low, but that shouldn’t have any effect on the vaccinated group. See Name link.
So it’s entirely possible that a strain in Israel has now mutated to avoid the protection of the vaccine from serious disease, and will soon work its way over here. Will this ever end? It may not be vanquished in our lifetimes. It looks like remote work and large suburban homes may stay in vogue for quite a while.
Agree 100%. As best I can tell, JtK is trying to make some sort of point that natural immunity is better than a vaccine. He’s wrong.
The benefit of vaccine induced immunity is your body becoming preemptively aware of the anti-gen without going through the overhead of suffering and in some cases death. Otherwise, natural immunity is just the same as Vaccine induced immunity.
Vaccine just presents the blue-print of the disease (anti-gen) with its replication capability removed (mRNA / protein sub-unit technologies), neutered (inactivated virion) or limited (adenovirus based).
Depending on the fitness of the individuals immunity system, it is possible natural infection may induce BETTER immunity because of exposure to host of differences/mutations/random differences in the virus particles. But at a community level determining fitness of each individual is not trivial and therefore mass vaccination becomes preferable.
Ideally we want our species to genetically evolve so we can defeat disease naturally. Vaccination is a viable in-between where it has been proven to be safe, effective with a complete understanding of the disease and its mutants.
This article in Nature provides a good summary of the issues. They do quote the Israeli study showing what could be a drop in vaccine effectiveness:
“Last month, the Ministry of Health in Israel, a country that has one of the world’s highest vaccination rates, released raw data on vaccinations and infections from December 2020 to July 2021. The ministry estimated that vaccine protection against both infection and disease had dropped from above 90% in the early months of its programme to around 40% by late June — a decline that could be due to the effects of the Delta variant.”
And the last slide from the Israeli MIH does breakdown the estimated Vaccine Effectiveness by month of second dose, which does appear to drop down month by month. (Though I can’t read Hebrew so there may be some relevant statements in the text which I’m missing)
Additionally, “…analysed health records from more than 1.3 million people who were vaccinated between January and April 2021. Those vaccinated in January and February were 53% more likely to test positive for SARS-CoV-2 during those four months, compared with people vaccinated in March and April. The differences were even starker among the earliest and latest vaccinated.”
But the Nature review also points out that there could be confounding factors here. The first people to be vaccinated were more likely to be health care workers (who have high chance of exposure) and the old and sick. Also there could be behavioral issues with people getting pandemic fatigue and engaging in more risky behavior after being vaccinated for a while.
B-Cell memory is kind of permanent. It can survive several decades if not the whole time life. “Falling efficacy” is perhaps another term for changing variant. Delta+ is now taking over.
Also, these terms “Delta”, “Alpha” etc are broad based. This virus is always changing. There are literally thousands of recorded variants. The broad-based terms are kind of catch all for superset features of these variants. Every time, every single viral particle when it replicates, undergoes some change.
And all kinds of changes take place during mutation that B-cells may not recognize. While the body is learning about this ‘new’ anti-gen (2-3 days), in some people that might be long enough for viral overload enough to make their situation worse. If after the viral overload, the body is unable to mount a viable immune response or doesn’t receive the appropriate external care (anti-virals etc.,) depending on the severity of infection outcomes can range from extreme distress to death. If however, the body is able to mount a viable immune response, the individual should be able to clear the infection with some or no distress.
Any remaining efficacy, in my view is likely to come from partial recognition of the mutated anti-gen or was infected with multi-variant – where variants are competing for replication/mutation surface within the host. Vaccines are life-savers. But they too have their limitations when dealing with a dynamic process within a dynamic system.
This is why vaccine or not, one really should keep their immune system in tip-top shape.
“Falling efficacy” is perhaps another term for changing variant. There is probably different efficacy against different variants. But the Israeli study and others are specifically looking at efficacy change over time.
In my laypersons understanding while breakthrough cases are expected if there were no time component to efficacy (the null hypothesis) then those cases should be evenly distributed with respect to how long ago a person was vaccinated. If you sort breakthrough cases by time since vaccination and find that cases are disproportionately likely in those vaccinated longest ago, that could indicate that vaccine efficacy declines over time. Or it could be some of the confounding factors mentioned by the Nature article. Or there could be some other design/statistical flaws in the study.
ADE (Anti-body Dependent Enhancement) is a phenomenon where immune system that is aware of strain S1 is fooled by strain S2 camouflaged as S1. But once S2 gets inside white blood cells (macrophage), the immune system isn’t prepared to deal with the real S2. Then S2 goes on about its destructive business.
This has been most commonly observed in humans with Dengue virus which is also a RNA virus.
For this reason, in addition to vaccines it is very important to have a treatment protocol in event of breakthrough infections or unexpected outbreaks in unvaccinated populations. Also why it is important people maintain social distancing and masking despite being vaccinated in the current environment. In addition to doing everything to keep their respective immune systems in great shape.
There is this skewed notion that vaccines are ‘one and done’. It is not so with a globally highly active/mutating RNA virus such as Covid. Dengue is even more lethal, but is limited by its transmission vector (mosquitoes).
It is extremely difficult to develop safe, reliable and long lasting vaccines. It is also unfair and unfortunate for the current episode to have assumed unsavory political hue.
1. Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies (nih.gov)
2. Long term evolution of SARS-CoV-2, 26 July 2021 (gov.uk)
ADE is not driven by vaccine. ADE is driven by lack of vaccinations. there is new data showing this is also the case with Covid: Full vaccination suppresses SARS-CoV-2 delta variant mutation frequency (medrxiv.org)
Antibody-dependent Enhancement (ADE) and Vaccines (Children’s Hospital of Philadelphia)
A couple of key paragraphs from the cited page that you might have missed, emphasis added:
“Both the [Respiratory syncytial virus] and measles vaccines that caused ADE were tested in the 1960s. Since then, other vaccines have successfully been created by purifying and chemically inactivating the virus with formaldehyde, such as hepatitis A, rabies, and inactivated polio vaccines. These more recent vaccines do not cause ADE.”
“Neither COVID-19 disease nor the new COVID-19 vaccines have shown evidence of causing ADE. People infected with SARS-CoV-2, the virus that causes COVID-19, have not been likely to develop ADE upon repeat exposure. This is true of other coronaviruses as well. Likewise, studies of vaccines in the laboratory with animals or in the clinical trials in people have not found evidence of ADE.”
So durable that Israel is now requiring a third “booster” shot. I am sure this is just to reinforce the existing amazing durability. The US (Dr.Fauci) is now recommending (mandating?) third shot for immunocompromised. But don’t worry that’s just the immunocompromised right? Dr Fauci says the following on that: “We are already starting to see indications in some sectors about a diminution over time” in vaccines’ durability… Make your appointments now!!
Durable doesn’t mean indefinite and booster shots are nothing new nor specific to the COVID-19 vaccine. To more fully quote Dr. Fauci:
“No vaccine, at least not within this category, is going to have an indefinite amount of protection…inevitably there will be a time when we’ll have to give boosts.”
That’s particularly true if the virus is allowed to spread and further mutate due to low vaccination rates and poor adherence to simple preventative measures, such as masking.
And with respect to boosters for immunocompromised individuals, “giving them an additional shot is almost not considered a booster, it’s considered part of what their original regimen should have been,” as vaccines rely on an immune system response, which is compromised for immunocompromised individuals, to produce antibodies.
Yes, when you talk about the small subset of hospitalized people in an exceptionally well vaccinated country, the percentages from that small subset will be high. Every last one of these reports also states something to this effect: “The vaccine was 91% effective at preventing severe illness in the same period between June 20 and July 17, the ministry said.”
I’m really not sure what folks think they’re doing on here with these incomplete takes. Fun with stats in real estate is one thing. A pandemic though? I personally find it really lousy and I’m surprised they aren’t summarily deleted, to be honest.
people just don’t understand stats and math. i think that has been clear from this pandemic. we need much more education in stats in high schools. of course there are people “playing” with the numbers to support their message, but a lot of people are just uneducated.
Interesting take. I imagine that if you really built in statistics into American life then our behaviors would be wildly different. Gun violence, traffic accidents, cancer, and heart disease would be at the front of the show. Oh, and COVID with a dull 1/500 chance of death in the US — unfortunately much higher than many other much less wealthy counties. You can make obesity and ethnic arguments, but the truth is every human is unique and we have quite the set of variants in the mix.
Oh, and how do you obtain statistics on a new variant in the middle of a worldwide epidemic? Without universal health systems?
Well, I think the answer to that for most people in the US is unfortunately random unsupported thoughts on social media.
Meanwhile Texas, Florida, Arkansas, Missouri, Louisiana, Arizona are in dire need of medical staff and supplies again. Is there a more powerful statistic then that? Note that this also means infected people aren’t getting the care they need — perfect fertile ground for new variants to evolve. A 50/50 population split on vaccinations is quite the experiment design for vaccine breakthrough strains. If only our messaging had been about statistics of protection via vaccine …
People would have still ignored said messaging because “Lie-burals” or “Big Pharma” or “Jesus will protect me” in said Talibanesque states
From the Nature article: “But what’s unclear is whether relatively mild infections among vaccinated individuals being observed now are a harbinger of further loss of protection, says Aldridge. “Is that an early warning sign? That’s what we don’t know.”
This is why people are looking at this.
What I want to know is why no one–UC, CDC, whoever–seems to be doing truly random sampling, either of antigens or antibodies. Both would be interesting. For example, I’d like to know what percentage of the unvaccinated population has antibodies from prior infection and therefore can be added to the vaccinated number to arrive at a total proportion of the population with some immunity.
“Early indications suggest that antibody levels triggered by most COVID-19 vaccines are falling, too. What scientists don’t know is whether these drops reflect a decline in protection against the virus. Teams around the world are racing to determine what level of neutralizing antibodies or another immune marker is most closely associated with a vaccine’s effectiveness. They’re seeking what’s known as a correlate of protection.”
People are looking at this. But it seems like what they don’t know is how antibody levels correlate with vaccine effectiveness.
78% of all COVID hospitalizations and deaths are for people who are obese or overweight, per the CDC.
People would benefit in so many ways by eating healthier and getting more exercise.
Amen. At this point, obesity is a way bigger health risk than covid for most of the population. And the lockdowns greatly increased obesity.
How communicable is obesity?
If the cost of high quality food (whole complex carbs, lean meats, green veggies, protein variety etc) is increased and cost of low quality food (simple sugars, fatty meats, limited proteins) is decreased — current situation, then there will be natural selectivity towards obesity – because of survival imperative.
If cost of high quality food increases to such a level that it is practically inaffordable, and sources of income are limited to sedentary jobs requiring long hours with limited outdoor activity, then cultural/social practices around obesity become normalized, acceptable and communicable (replicating social behavior). Communicability of disease is as much a cultural emergence as it is biological. Environment begets culture which begets biology — the nurture part.
It may be NOT as highly and obviously communicable as a highly infectious RNA virus — but its communicable. I mean even for this disease/virus, its really the environment of availability of large number of hosts that makes it communicable.
If you want to solve for this virus, good diet/exercise can absolutely help. There are several dynamic and complex factors at play — casting it simplistically as pressing this “BIG RED” button will solve, is in my view, is not helpful.
If you want to solve for this virus, wear a mask and get vaccinated. Period.
Look, this is a non-equilibrium virus. That is, it jumped between species (bats to humans) and it hasn’t yet established a long-term co-survival relationship with humans (cold virus is an equilibrium virus). It may or may not have been initially enhanced for human infectivity – but it has shown great capacity for mutation assisted virulence and lethality in wild. Also it has managed to jump to additional species besides humans – minks, ferrets for ex. And its possible it can propagate to even more mammalian species. Which means (in my view) it will progress to an endemic virus. Even without jumping to other mammals, it has an extremely large mutating surface in humans. The only hope is that it and we can quickly figure out a long-term co-survival relationship.
Sure, it jumped between species. It might become endemic. But right now, the most important thing is to get vaccinated.
UPDATE: COVID-19 Hospitalizations Hit First Wave High in San Francisco