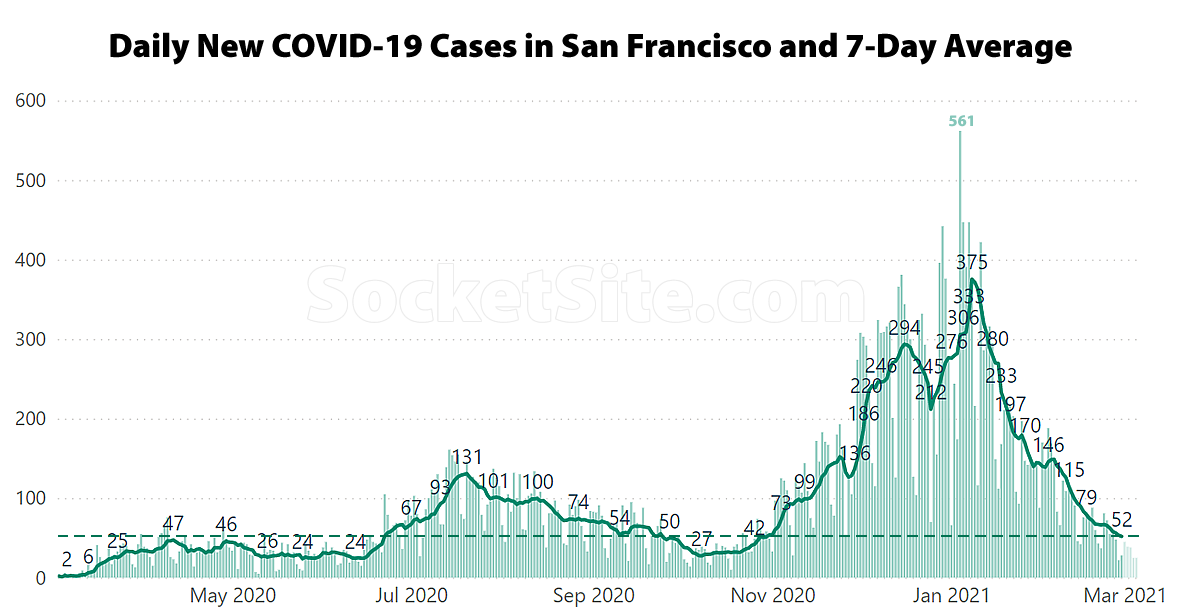
Having hit a revised pandemic high of 375 on January 8, the 7-day average number of daily new COVID-19 cases diagnosed in San Francisco has dropped to 52, which is the lowest 7-day average since the end of October, 2020, with a percent positive rate for those who are tested having inched down to 1.22 percent, which is a 4-month low as well.
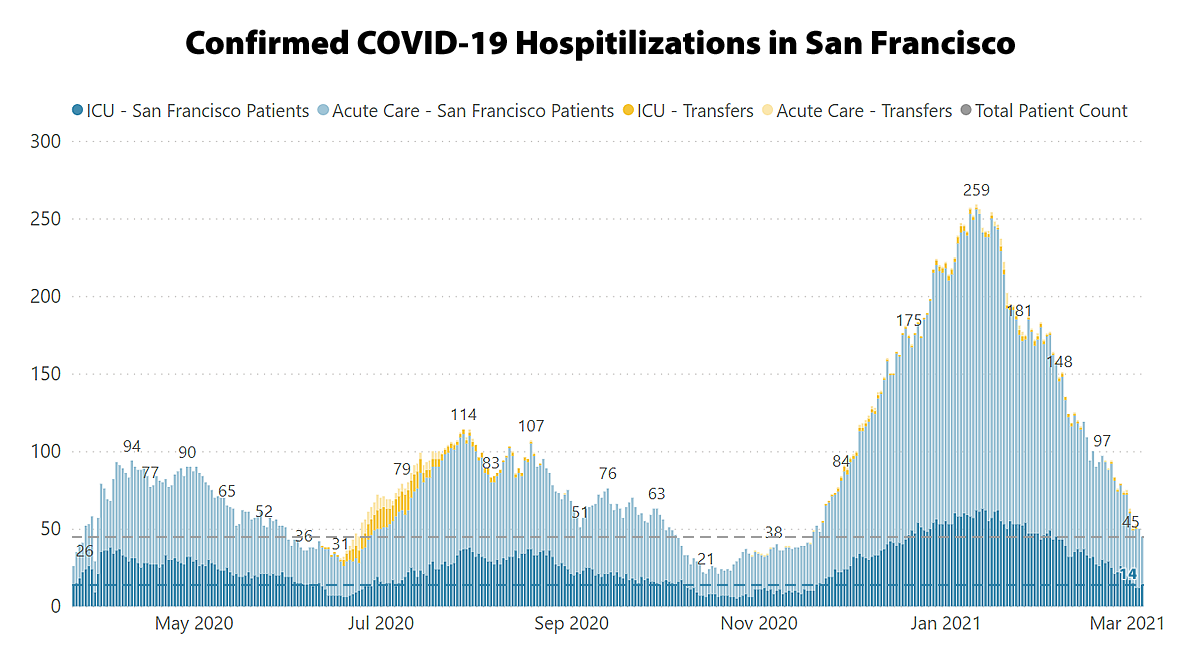
Local hospitalizations have dramatically dropped as well, but there are still 45 local hospital beds occupied by COVID-19 patients and at least 14 people in an ICU.
And with the adjusted average COVID-19 case rate for San Francisco, which takes into account testing rates, having dropped under 4.0 new cases per 100,000 residents per day, the city’s assigned risk level could drop from Substantial (Red) to Moderate (Orange) in two weeks time, which would allow for additional business reopenings, capacities and indoor activities as well.
And as such, please continue to keep the masks up and the numbers down.
UPDATE (3/23): As projected, San Francisco’s assigned risk level has just dropped from Substantial (Red) to Moderate (Orange), allowing for offices, outdoor bars and indoor recreational facilities to reopen, with capacity restrictions, starting tomorrow, March 24 at 8:00am.
More specifically, non-essential offices can operate at up to 25% capacity and all bars and breweries can open for outdoor service. Outdoor arts, theater, music performances for audiences of up to 50 people will be allowed beginning April 1. And capacity restrictions for activities already opened, including all “retail, personal services and equipment rental, outdoor and indoor dining, outdoor and indoor fitness, indoor religious activities, indoor movie theaters, museums, zoos and aquariums, and open air bus and boat tours” will be expanded, typically up to 50 percent.
With the CDC officially endorsing small indoor gatherings of maskless vaccinated people, I am hopeful that we can finally staunch the bleeding of small bars and restaurants.
* “federal health officials advised that fully vaccinated Americans can gather indoors in private homes in small groups with other fully vaccinated people, without masks or distancing”
You omitted a few details (see), but yes, anything would be an improvement over what we’ve had for 354 days.
Based on the CDC’s own peer-reviewed report published last Friday which analyzed 3,142 counties from 3/1/20 to 12/31/20, masks reduced cases by 1-2% at best. Considering the questionable case reporting, its fair to say that masks had little to no benefit. But of course people only “trust the science” if it aligns with their opinions.
In terms of the actual impact and benefits:
“Mask mandates were associated with a 0.5 percentage point decrease (p = 0.02) in daily COVID-19 case growth rates 1–20 days after implementation and decreases of 1.1, 1.5, 1.7, and 1.8 percentage points 21–40, 41–60, 61–80, and 81–100 days, respectively, after implementation,” and a “0.7 percentage point decrease (p = 0.03) in daily COVID-19 death growth rates 1–20 days after implementation and decreases of 1.0, 1.4, 1.6, and 1.9 percentage points 21–40, 41–60, 61–80, and 81–100 days, respectively, after implementation.”
And the key insight(s):
“Mandating masks was associated with a decrease in daily COVID-19 case and death growth rates within 20 days of implementation. Allowing on-premises restaurant dining was associated with an increase in daily COVID-19 case growth rates 41–100 days after implementation and an increase in daily death growth rates 61–100 days after implementation.”
“In March and April 2020, 49 states and DC prohibited any on-premises dining at restaurants, but by mid-June, all states and DC had lifted these restrictions”
News to us !!
(and which WAS the holdout state??)
But when you look at the p values and the CI’s and the numbers involved its just statistically meaningless noise. Hardly surprising as only N95/N99 respirator masks have been shown by substantive research to have any measurable impact on transmission of viral respiratory illnesses where the primary mode of transmission is tidal breathing aerosols < 2 micron. Cotton masks are placebos, N20 surgical masks have no real effect unless properly seated. Now when the primary symptoms are sneezing or wet coughs, thats a different matter. But SARs CoV 2 has neither.
So a monumental waste of time. And thats the actual science. Far Eastern researcher have published lots of interesting papers on the subject in the last few decades.
And all for something with an IFR of < 0.02% and very high cross immunity. Which is H1N1-09 ballpark numbers.
Has anyone checked out the CDC VAERS numbers recently? For the SARs CoV 2 vaccine adverse reactions. A very sobering read. Especially when you compare them with the Influenza vaccine numbers for the last 30 years. That's a lot of old dead people. Especially those with dementia. No informed consent there.
[Editor’s Note: Do not leave this page without reading our reply.]
That’s factually incorrect. The p-values, as provided, are statistically significant. And more importantly, and directly from the CDC:
“Over 92 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through March 8, 2021. During this time, VAERS received 1,637 reports of death (0.0018%) among people who received a COVID-19 vaccine,” but “a review of available clinical information including death certificates, autopsy, and medical records revealed no evidence that vaccination contributed to [any of the aforementioned] patient deaths.”
Or quite simply, “VAERS has not detected patterns in cause of death that would indicate a safety problem with COVID-19 vaccines,” despite some spurious misreports, based on misrepresentations of the data, to the contrary.
At the same time, over 526,000 people in the U.S. have died from COVID-19 over the past year, with over 54,000 deaths in California alone.
I respect SS editor’s opinion about not deleting the post but I’m in favor of deleting.
Where to even start? Claiming that N95/N99 masks are not effective is flat out false. There have been many studies on droplets and aerosols with coughing, sneezing, speech, and normal breathing. tfourier cites particles <2 microns but N95/N99 are tested to 0.3 microns. And they actually capture particles smaller than .3 microns better but .3 microns is the hardest size particle to capture. (google something like brownian motion/particle size if curious). And then s/he seems to imply that surgical masks might do something if properly seated while s/he claims N95/99s do nothing? This is self-contradictory.
Re: infection fatality rate <.02%… No one knows the actual CFR/IFR. There have been many studies and it is lower than taking the literal 1.8% from the JH dashboard. No one knows the correct ascertainment bias but there are several machine learning models on the total denominator as well as multiple other studies and CDC figures. If I had to guess, I'd put it at around .40% vs tfourier's <0.02%. I've never read a study with it that low. Maybe it exists but it would be an extreme extreme minority opinion. As far as other people claiming that it is less deadly than the flu- that is also false esp as the flu also has asymptomatic cases.
"Very high cross immunity." assuming s/he i s talking about the theory that because some colds are coronaviruses and thus if you have had a cold in your life you might have immunity. That theory was examined in the ?fall of last year? Don't think many scientists believe that now- especially as immunity in people who had covid itself is failing against variants. (And the most recent study had 10% of people with covid not even having adequate immunity to the same virus(not a variant)).
His main point seems to be fabricating numbers to say covid isn't deadly and people have high immunity from the common cold to it. Dismissing something that has already killed over 500,000 people in the US is terrible and doing it with lies is more reprehensible. Btw, in the majority of epidemics/pandemics, the deaths are underestimated and revised higher years later.
His/her comment about VAERS is just a flat out lie.
I get free speech and respect the editor's opinion, but this is just nasty stuff. There is no way tfourier believes this stuff. The comments about "a lot of old people…. esp with dementia" is just intended to generate doubt and misery for people whose parents are getting vaccinated.
Normally I'd say don't feed the trolls and I wouldnt reply but I found this comment dangerous and nasty and someone will read this and think- oh this person uses acronyms and sounds pseudo-scientific- I'm not going to wear a mask or get vaccinated. There are a lot of things we still don't know about covid, but the impact of wearing a mask is not of them. In another forum, I saw a software developer put together a tool to show that masks actually made covid worse. I went into the github and he was comparing single point in time surveys about mask wearing vs cumulative deaths to a different date to do a simple linear regression. Super basic problems there from a stats 101 standpoint, but people see that and will believe – oh this looks scientific- masks are bad. There is a growing dissonance between what we know and what we think we know as long as we can garner a few key words and acronyms from the interwebs.
This whole thing is "a monumental waste of time. And thats the actual science."
Amen.
WSJ: Russian Disinformation Campaign Aims to Undermine Confidence in Pfizer, Other Covid-19 Vaccines
Looks like it’s working!
completely incorrect. socketsite, suggest deleting anti-vax messages like this.
Agreed. Moronic economics takes are de rigueur here, but quack epidemiology should be out of bounds.
Agreed. Disagreeing about zoning regulations is fine. Allowing anti-vax b.s. is life threatening to vulnerable populations.
There’s also no reason for this website to do the Russians work for them.
Take it down.
We believe in countering misinformation with facts, particularly at a time when the VAERS data is widely being misreported and mischaracterized.
Countering misinformation with facts works in a debate.
That’s not what this is and that’s not how misinformation functions on the internet and anonymous commentating. It becomes both-sides-ism. Real science textbooks don’t give equal time to Creationism.
Now it the time to actually use editorial discretion.
Reduction of 1-2% is not change in total cases, but in growth rate. You have to take the “natural log” of daily cases and calculate the difference to get the % difference in growth rate as it explained in the article. This means that 1-2% change in growth rate is quite significant (given how many cases in the counties).
UPDATE: As projected, San Francisco’s assigned risk level has just dropped from Substantial (Red) to Moderate (Orange), allowing for offices, outdoor bars and indoor recreational facilities to reopen, with capacity restrictions, starting tomorrow, March 24 at 8:00am.
More specifically, non-essential offices can operate at up to 25% capacity and all bars and breweries can open for outdoor service. Outdoor arts, theater, music performances for audiences of up to 50 people will be allowed beginning April 1. And capacity restrictions for activities already opened, including all “retail, personal services and equipment rental, outdoor and indoor dining, outdoor and indoor fitness, indoor religious activities, indoor movie theaters, museums, zoos and aquariums, and open air bus and boat tours” will be expanded, typically up to 50 percent.