Having rolled back the reopening of all indoor dining last week, and re-reduced the allowable operating capacities of fitness centers and movie theaters, San Francisco will now roll back the reopening of all non-essential offices, which were allowed to reopen last month, and further reduce the allowable capacity of fitness centers and gyms to 10 percent of max, effective Tuesday, November 17, 2020, and due to a continued increase in COVID-19 case rates.
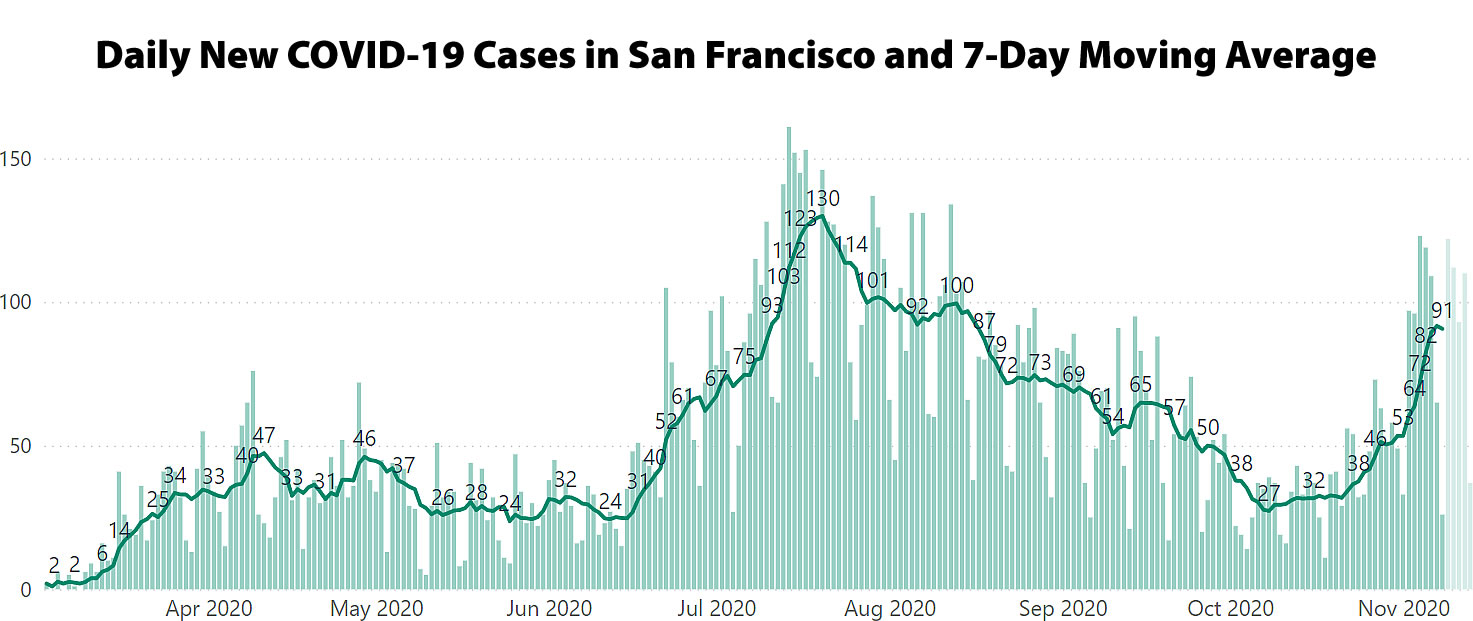
The number of new COVID cases in San Francisco, which is still climbing, has jumped from an average of 27 cases per day in early October to over 90 cases per day as of last week, with the case rate having increased from 3.1 cases per 100,000 people to 10.4 cases per 100,000 people and versus a target of under 2.0 (1.8 to be exact).
UPDATE (11/23): While preliminary and likely to be updated (up), the number of new cases diagnosed in San Francisco on 11/16 (161) matched the previous one-day high set in mid-July. The local 7-day average of new cases is back above 100 for the first time since August and hospitalizations are up nearly 30 percent over the past week.
UPDATE (11/24): The number of new cases diagnosed in San Francisco on 11/16 has been upwardly adjusted to 164, representing a new one-day high and pushing the 7-day average of new cases up to 110 (which is the highest moving average since late July).
SF is still doing better than the rest of California which in turn is doing better than the rest of the USA. So much for the idea that living in a dense city increases the risk of contracting covid. The Dakotas are three times riskier than California.
I worry about the future of fitness studios as many of their patrons have learned how to stay fit without a $100/mo. subscription fee.
There is a huge disparity within the state, too. San Diego County is on a Dakotas-like trajectory. It’s possible that California will turn out to simply be later, rather than better.
Right. The spread of a disease like this is like how California wildfires spread. The fuel is people and prevention measures like lock-downs are akin to containing and extinguishing wildfires. All that fuel left on the ground will eventually burn sooner or later.
The main difference is that a vaccine can render the “fuel” to be non-flammable.
Now this is entirely anecdotal and largely uninformed. A scientist friend of mine warned me that given the vectors and rate of contraction it is inevitable that everybody is going to get infected. The whole point of mask/lockdown was to keep the infection curve flatter (as opposed to steeper) within the timeline to avoid overwhelming the healthcare capacity.
It is entirely possible many of us have already been infected and progressed to survival without any outward symptoms. The numbers on the graphs may only reflect those who have ‘tested-positive’ post symptom exhibition but its really not the true number of infected in my uninformed and unqualified opinion.
Surely you have other places to talk about this stuff.
?? Cave Dweller is on the topic of the post, which is COVID-19.
I think the point is to not bring up what was brought up eight months ago – almost word for word – although I suppose the defense of reminding people of the basics can be offered. And given the number of people who seemed to have never learned the material in the first place, – “Lol, I love this teachable moment wrapped in sass. Learn” – I can’t say I disagree.
Technically the topic is the re-closing of businesses, which is economic news.
Now, whatever his scientist friend actually said, his interpretation of it is nonsense and it is bad health advice worthy of a russian troll. The vaccine works and you just have to hang on for another six months and do what you can to support essential workers.
The speculation that we have all had it already has been bouncing around since march, at which point it was a reasonable question. At this point it’s mostly favored by people who are looking for an excuse not to wear a mask. Whatever the antibodies say, the deaths are rising, so if we’ve all had it already that doesn’t appear to be doing us much good. So why bring it up?
Both of Cave Dwellers points are not just wrong but dangerously wrong. But my point is that nobody should be taking my advice on this either. There are verified medical professionals blogging and tweeting with their real reputations at stake. You want to play armchair epidemiologist over a beer with friends that’s one thing, but if you know you’re uninformed you shouldn’t be spreading uninformation. I’m sorry if this is harsh but people are literally dying from weaponized BS right now.
Heynonnynonny: Very well said, agree 100%.
Don’t get your health/medical advice from real estate sites.
If its the truth and facts then one shouldn’t be sorry that the delivery is harsh. In Cave Dwellers world we prefer harsh blunt truths.
Here is another point of view. Lets say it takes some amount of time before efficacy of the vaccines are established beyond lab testing and in large numbers. And lets further speculate it takes some more time to figure out the logistics of manufacturing, distribution and delivery across a wide swathe of population up and down the nation. So if we agree that it takes X amount of time between general availability of an effective vaccine and the time it takes to quell the infection, would you say that we are likely to experience more infection spikes and related economic lockdowns before we return to a stable/healthy situation? In your view, what do you think is that X time?
And what does that mean for SF RE? Several companies have already pushed out ‘back-to-office’ dates out to Sept 2021. What do you think will be effects on rental market?
If a company can achieve sustainable productivity with WFH, do you think we could see formalization of such a model in the years ahead? If you agree with this, what do you think would the be long term economic effects for SF and the Bay Area in general?
Science Magazine ‘Just beautiful’: Another COVID-19 vaccine, from newcomer Moderna, succeeds in large-scale trial
“Obviously, the data speak for themselves,” says Anthony Fauci, head of the U.S. National Institute of Allergy and Infectious Diseases (NIAID), which helped support the study. “This is a very positive result.” He suspects that by late next month doses of one or both vaccines could start to be offered to people at highest risk from SARS-CoV-2, the virus that causes COVID-19.
But many questions remain about the durability of the vaccines’ protection, their safety, what FDA will demand to approve them, and the challenge of rapidly producing and distributing hundreds of millions—if not billions—of doses. For example, because warm temperatures cause the RNA and lipid particles to degrade, the vaccines must be kept frozen until days before use, requiring a “cold chain” to move them from manufacturing plants to pharmacies and clinics.
Ruth Karron, who heads the Center for Immunization Research at the Johns Hopkins Bloomberg School of Public Health, notes that neither Moderna nor the Pfizer/BioNTech study evaluated whether the vaccine prevented infections as well as symptomatic disease, which is key to controlling the spread of the virus. “The data we have are that these vaccines protect you against severe illness, but it doesn’t mean that you can’t get infected and give it to your patient, your neighbor, your customer, or whomever,” Karron says.
Six months, you said heynonnynonny? or care to explain that timeline?
It seems MRNA has given up all their gains since the announcement of their “94.5%” efficiency number. Would you happen to have any idea why the market thinks this stock is overvalued? I am genuinely curious about your optimism around vaccines.
You need to get past the headlines and hot takes.
The drop was driven by an analyst recommending some profit taking and reducing his rating to “market perform.” At the same time, the same analyst increased his price target from $94 to $109 per share (which most people missed and is 11 percent above yesterday’s high and 17 percent above its current price).
In the words of the analyst: “We believe a near-term best-case scenario is mostly reflected in shares, including an mRNA-1273 EUA before year-end and full approval mid-2021.”
And now back to the topic at hand…
because Moderna is significantly overvalued, even if they succeed wildly. They are valued higher than fast growing biotechs with multiple products on the market. Look at their 9 month chart. it’s nuts.
the current estimate is that 3-5x the number of people have been infected over those tested positive. In SF, that would still leave our rate below 8%. everyone will not be infected if we continue on a partial shutdown and wear masks. I think we can keep our SF rate below 20%. health care workers will get vaccinated in Dec-Feb, elderly in Jan-March, and the rest of us by summer.
Now the midwest is another story altogether and likely 40-50% will end up infected.
each group of vaccinations will lower the Rt and help control spread. We just need to hunker down hard for another 3-4 months, and hunker down soft for an additional 3. Summer is looking good.
Speaking of dense cities, this is what happened in Tokyo:
Six hundred fifteen healthy volunteers (mean + SD 40.8 + 10.0; range 19-69; 45.7 % female) received at least one test. Seroprevalence increased from 5.8 % to 46.8 % over the course of the summer. The most dramatic increase in SPR occurred in late June and early July, paralleling the rise in daily confirmed cases within Tokyo, which peaked on August 4.
Cases are a stupid measure. Only hospitalizations and deaths matter as cases are simply a function of testing level. In any case, this will only kill more small businesses. Can’t wait to get out of here after 20+ years and a California native. SF is a disgrace now.
It’s true that cases alone are not the right measure to look at in isolation. But SF’s percent positive rate from testing has doubled from less than 1% a few weeks ago to 2% this week and it’s not clear whether it’s plateaued or will keep climbing, and hospitalizations have also gone up by close to double in that time as well. That said, SF’s overall positivity rate and hospitalizations are still substantially below what they were during the summer case surge and not too bad overall. Of course hospitalizations and deaths tend to lag cases by a couple weeks. But if your only measure of things getting bad is death, that’s a pretty low bar considering the mounting questions on longer term effects of COVID for many people, and the surge on the hospitals with COVID patients would be bad news for people potentially dying of other preventable things even if the COVID patients survive. Once a vaccine is available at least for highest risk people (eg seniors, health care workers, essential workers), then I think more opening up will happen.
While average daily testing volumes in San Francisco have increased 12 percent from early October to today, the average daily case rate has increased 235 percent over the same period of time.
Deaths are an appropriate measure when taking such draconian action as shutting down the livelihoods of millions of people. I understand that many of the folks proposing these shutdowns are largely immune from the consequences of such devastating actions. Real people however are left unable to pay the rent or feed their families. All the while the ruling elites ignore the orders that pertain only to the little people. They continue to go to parties and hold gala affairs. These shutdowns are nothing more than monumental ignorance brought about by unbridled arrogance. WTFU
death is not the appropriate measure. hospitalization are serious consequences and many of these people have long term effects. that hurts the economy too. Im sure if you were hospitalizes, intubated, survived and then had long term serious lung and heart and CNS effects, you would feel differently.
So Jimbo deaths are not an appropriate measure?
No. There have been significant advancements towards saving lives, but they require a hospital stay. If hospitals fill to capacity, then death rates rise for those who were denied treatment. So, knowing the numbers of rising Covid related hospitalizations is the most important measure.
And while lagging around two weeks, hospitalizations, which have just started ticking back up, tend to be correlated with overall case rates.
The case fatality rate for covid in the USA is about 2.2%. The death per 100k is about 72. For perspective cancer deaths per 100k is about 162
Cancer isn’t contagious.
Of course cancer isn’t contagious that was not the point. The point is the level of death associated with covid is less than many other maladies. Where a mask social distance wash your hands, but keep the economy open. We are delusional if we think we can lock ourselves down every time the infection rate spikes.
i dont think you understand exponential math. this could quickly spiral out of control like it has in the midwest, france, UK, Italy, Belgium and sweden, whcih have all announced almost complete lockdowns
I also don’t think you understand “novel virus.”
i truly do understand it. I’m a research scientist (neuro) with an MPH from Hopkins and have spent 25 years in biotech working in drug development. Not a vaccine expert by any means, but can assess the science very well and lucky to have immunologists and infectious disease experts.
this virus is novel, but the structure of the spike protein and lack of significant mutation make it a relatively easy target (unlike seasonal flu and HIV for example). we now know that targeting the spike protein works and have 2 vaccines with >90% efficacy. durability is a question but we know almost certainly it will last at least a year, but probably longer.
the next 3-4 months will be hell, but then we will get relief and relative normality by the Fall (if not sooner)
Sorry Jimbo- my novel virus comment wasn’t directed at you but towards JtK’s comment about low CFR.
And once the virus grows beyond the capacity of hospitals to be able to treat the seriously ill, those numbers will grow.
True, cancer is not contagious but Covid is and people with cancer and other risk factors have even higher chance of dying from Covid compared to the general population.
I guess everyone has their own threshold of how many people’s lives vs livelihood are worth saving. There is a balance but there is no 2nd chance after somebody dies.
Economic support is needed to help those with compromised economic livelihoods the next few months to get the vaccine to front line workers and the immunocompromised. This is achievable over the next 3-6 months and there is a light at the end of this tunnel where we can minimize death rates and economic impact but the current hopefully final Covid wave is going to test our resolve to find this balance that feels like a step back when we are actually moving closer to the finish line.
yes everyone has their own threshold. Those that are well protected by wealth and stay at home jobs believe that a relatively remote chance of death justifies almost any deprivation on those who are not.
are you suggesting we open up so poor people can die?
That is an interesting point. Who is actually dying from covid? Yes of course those on the lower socioeconomic scale are harder hit, as they are with all health outcomes.
But it is really the cohort over 80 years old, often with comorbidities, that is bearing the bulk of the deaths. They represent 41.1% of all deaths in California. 18-34 yrs old account for just 1.6% of the deaths.
So yes they should go back to productive work. Borrowed funds are just a tax on future earnings. We all know who will end up footing that bill. Hint it wont be Google Amazon Facebook and twitter!
The bulk of the deaths, 57 percent, are actually spread across the cohorts you don’t mention (6 percent 35-49; 19 percent 50-64; 33 percent 65-79), with those under the age of 50 representing 70 percent of the overall case load and the largest cohort of potential spreaders/carriers.
a large stimulus would mostly take care of this problem
A debt funded stimulus is a “tax” on future earnings. Who do you think will pay that “tax”?
Then stop thinking of it as a “stimulus” and call it what it is: disaster relief. We aren’t trying to recover from a contraction in the economy caused by out-of-control banksters hawking dodgy ill-understood financial products blowing up, this is more like an act of nature.
This is a pretty mild rollback, the only activity eliminated is indoor dining. Lots of real estate aficionado/bartenders on here? Or little emporers of the corner booth awaiting their reascent to the throne?
Are converted bar condos going to be the new hot thing?
The data says that most spread is from personal gatherings, so the holidays will be rough.
That’s incorrect. The indoor dining rollback was last week. The rollback that goes into effect today re-shutters non-essential office buildings, as outlined above.
Regardless, the rollbacks have economic impacts which extend beyond those who directly rely on the rolled-back businesses for their incomes, such as those who collect mortgage payments and rents, both commercial and residential, from said income streams.
Then there’s the impact on commercial corridors, transportation and WFH considerations. And of course, bars have actually been shuttered since March while the Small Business Eviction Can [has been] Kicked Down the Road.
But sure, there’s nothing to see here.
Far more interesting than a change in non-essential office workers, is the estimated $1.6 billion dollars in back rent owed in California. A sizable sum which might interest those that rely on those golden streams for income.
Although between the size of that debt and the attitudes of the federal government towards both RE and securities, I think things will work out fine
Actually, considering that over 700,000 jobs in San Francisco proper are office based, we’d say the local rollback is not only far more interesting but more meaningful, in terms of modeling, as well.
was anyone going to non-essential offices anyway? i know we were allowing up to 25% occupancy, but i highly doubt it even reached 10%
Several tech companies have pushed back full office occupancy until Sept 2021. I am assuming that is in keeping in mind the optimism around vaccine and its efficacy. It seems to me for practical purposes 2021 will also be year of WFH if everything lines up and lock downs end. But to be honest, I think we are going to experience series of waves and related lockdowns until 2024.
A Doctor friend of mine opined that functional vaccine developments can take up to 18 months under the best of best circumstances when verified for efficacy, longevity and no adverse reactions. Typical vaccine development cycle takes several years (8-15).
This is all anecdotal and unqualified. But these guys International Federation of Pharmaceutical Manufacturers & Association appear to second that opinion.
your doctor friend has no idea what he is talking about
@jimbo — probably true. He claims to have only treated about 50-60 Covid patients with a death rate of approximately 1.5% in that part of the planet where infection rate is fairly rampant, lockdowns are not enforced and people wear their masks around their neck. He also managed to not get infected and win recognition from a national body for infection mitigation treatment procedures. But he is just one doctor from India. India’s COVID-19 cases have declined rapidly—but herd immunity is still far away, scientists say
Pfizer and Moderna who’ve been spending 100s of millions of dollars in the US probably know better.
it will certainly take >18 months to vaccinate all of India and much of the underdeveloped world, and we will have anti-vaxx idiots in the US to deal with too
I guess you are not allowed to reply to socketsite. I said the cohort accounting for the bulk of deaths are over 80 years old. Then I guess I am being “corrected”
when SS says the bulk of deaths are actually other ages… But SS is counting multiple age groupings and adding them up and pretending they are a single cohort. Of course 41.1% is less then 50%. But according to Hohn Hopkins the largest single cohort in California as they break it down is the grouping over 80 years old.
Once again, the bulk of the deaths in California, 57 percent, are actually spread across the cohorts you didn’t mention (6 percent 35-49; 19 percent 50-64; 33 percent 65-79), with those under the age of 50 representing 70 percent of the overall case load and the largest cohort of potential spreaders/carriers.
Yes. The single largest cohort is over 80 at 41.1%. It therefore goes without saying (although SS insists on saying it twice) that if you add up all the other age groupings it will total 58.9 %.
Got it! So “the bulk of deaths” in California have actually occurred in the cohorts of people that are under 80 years of age. And with that in mind, it’s time to get back to the topic and impact at hand…
We can do this all day but know this. My original statement is correct and stands as written. Adding multiple cohorts together in order to pretend you are contradicting my statement is a logical fallacy. For instance if I were to say folks over 75 (adding another cohort) accounts for 52.2% of all covid deaths in California. I would be correct. Does that fact invalidate what you said? What I said? No it does not.
What remains irrefutable is the largest single cohort is deaths over 80. No other cohort comes close. Therefore by definition this cohort constitutes the bulk of the deaths. There are a variety of other cohorts when added together are larger. I never claimed otherwise, though you are pretending I did, in order to give the illusion you are making a contradictory point. You are not.
Perhaps we shouldn’t have been glib, but there’s a rather important distinction between a cohort “bearing the bulk of the deaths,” as you originally wrote, and being the “largest single” contributor, as you have since rephrased (and included a “therefore” for good measure).
The former implies that this is primarily an issue about, and for, those who are 80 years old or older, which it’s factually not.
And we’ll hereby leave it at that.
We seem to have found the small intersection of QAnon adherents and socketsite commenters with this thread. Ugh.
My office (law firm) had announced over a month ago that there was no chance of even voluntary return to the office before April. I know most of the big tech companies have an even longer timeline. I wonder how many office workers/businesses this “rollback” will really affect. n=1, but I don’t know any non-essential worker who has stepped foot in any office over the past month (or since March).
UPDATE: The average daily COVID case rate in San Francisco has ticked up to 11.2 cases per 100,000, versus a target of 1.8 and up from 3.1 five weeks ago. And while trending down four days ago, local hospitalizations are now back on the rise (up 4 percent and climbing).
UPDATE: With the average daily COVID case rate in San Francisco continuing to inch up and local hospitalizations up 24 percent over the past week, and climbing, the county is poised to be reclassified as a “purple,” or highest risk, tier based on the State’s ranking system, which will require another round of rollbacks.
UPDATE (11/23): While preliminary and likely to be updated (up), the number of new cases diagnosed in San Francisco on 11/16 (161) matched the previous one-day high set in mid-July. The local 7-day average of new cases is back above 100 for the first time since August and hospitalizations are now up nearly 30 percent over the past week.
UPDATE: As expected, the number of new cases diagnosed in San Francisco on 11/16 has been upwardly adjusted to 164, representing a new one-day high and pushing the 7-day average of new cases up to 110 (which is the highest moving average since late July).